Understanding the specific ECG patterns of Brugada Syndrome is the first step in moving from a "hidden" risk to a managed condition. Since the heart's electrical activity is inherently dynamic and can fluctuate based on various triggers, medical professionals classify these visual signatures into three primary types to better assess a patient's vulnerability. These categories help clinicians differentiate between transient electrical variations and high-risk patterns that require immediate intervention. While Type 1 remains the only definitive diagnostic pattern, the dynamic nature of Types 2 and 3 requires specialized tests and increased vigilance. This guide covers the clinical standards in classification, frequency, and strategies for managing life with this syndrome.
The Clinical Spectrum: Type 1, Type 2, and Type 3
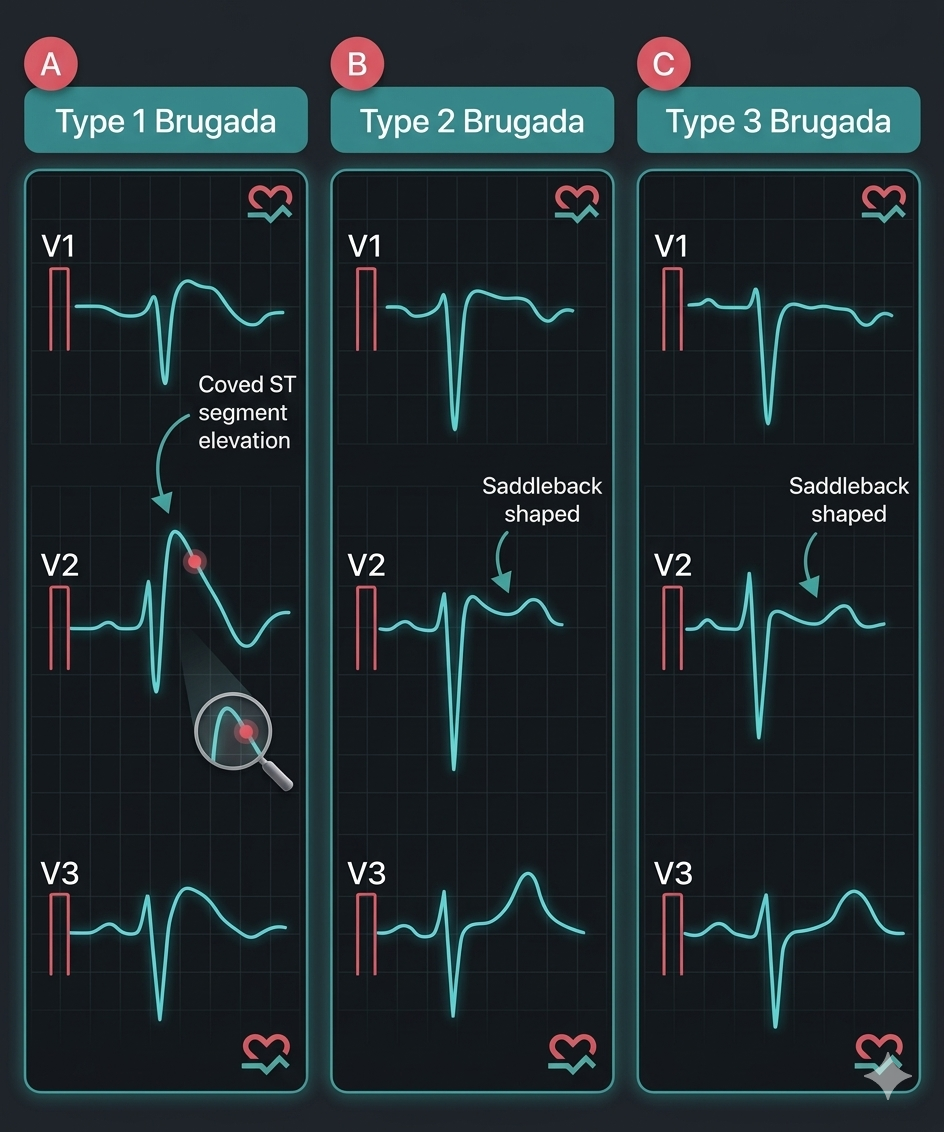
All three types affect the right precordial leads (V₁ to V₃), but their visual "signatures" tell very different stories about the heart's stability.
- Type 1 (Coved Type): This is the "malignant" pattern. It is characterized by a prominent ST-segment elevation ≥ 2 mm that descends into a negative (inverted) T-wave. A spontaneous Type 1 is the strongest predictor of future arrhythmic events.
- Type 2 (Saddleback Type): Recognizable by an ST-segment elevation ≥ 2 mm, but with a "dip" that looks like a saddle. The T-wave is usually positive or biphasic. While not diagnostic on its own, it is a significant clinical alarm.
- Type 3 (Intermediate Type): A "saddle" pattern where the ST-segment elevation is less than 2 mm (often < 1 mm). It is often seen in healthy individuals or athletes, making it the most difficult to distinguish from benign variations without additional testing.
Prevalence and Demographics
Brugada Syndrome is estimated to be responsible for at least 4% of all sudden deaths and up to 20% of sudden deaths in hearts that appear structurally normal on ultrasound.
- Asian Descent: Prevalence is significantly higher in Southeast Asia and Japan, where it can affect 1 in 700 to 1,000 people.
- The Gender Gap: Symptoms usually manifest in adulthood, peaking around age 40. Men are up to 10 times more likely than women to show the Type 1 pattern and suffer life-threatening arrhythmias.
The Diagnostic Challenge: "Catching a Ghost"
Because Brugada is a "flickering" condition, a normal ECG does not always rule it out. If a patient has a family history of sudden death or has experienced unexplained fainting (syncope), cardiologists use:
- Drug Provocation Tests: Administration of sodium channel blockers (such as ajmaline or flecainide). These drugs intentionally "stress" the faulty ion channels to see if a benign Type 2 or 3 will convert into a diagnostic Type 1.
- High-Lead ECG: Placing V₁ and V₂ leads higher on the chest (2nd or 3rd intercostal space) can sometimes reveal a hidden Brugada pattern that a standard ECG misses.
Management: Life After Diagnosis
Once a diagnosis is confirmed, the goal shifts to preventing an "electrical storm."
- ICD (The Gold Standard): For high-risk patients (survivors of cardiac arrest or spontaneous Type 1 with syncope), an implantable cardioverter defibrillator (ICD) is the only proven protection.
- Fever Management: Fever is a powerful trigger. Patients must aggressively treat even a mild fever with antipyretics to prevent sodium channel failure.
- Medication Avoidance: The use of specific medications (including certain antidepressants and anesthetics) is strictly forbidden. The website BrugadaDrugs.org is a crucial resource.
Night: The Window of Vulnerability
The link between Brugada Syndrome and sleep is well-documented. During rest, vagal tone increases, naturally slowing the heart rate. In Brugada patients, this physiological slowing can paradoxically trigger ventricular fibrillation.
This is where Cardiac Alarm serves as a critical secondary layer of awareness. Although it is not a replacement for an ICD, it provides an active monitoring system that does not sleep. By detecting a pulse drop below 33 beats per minute and activating a powerful siren, it ensures that a critical drop in heart rate during those quiet, high-risk hours does not go unnoticed — immediately alerting family members.
Key Action Steps:
- Check your latest ECG report and look for any mention of "Saddleback" (Type 2/3) morphology.
- Consult with an electrophysiologist (EP) about the need for a provocation test if you have Type 2 or 3 alongside symptoms.
- Activate Cardiac Alarm on your Apple Watch every night to ensure an audible safety net.
Important: This article is for educational purposes. Cardiac Alarm is an informational monitoring aid, not a medical device. Always follow the treatment plan prescribed by your cardiologist.